Form builder
Standard Assessment Tool — drag-and-drop, no code
Standard Assessment Tool
100%
Preview
Save
FORM ELEMENTS
Search…
▼General Information
Date
Time in
Time out
▼Client information
Client name
DOB
▶Service
▶Event code
▶Mileage
▶Reason for assessment
▶Patient history
New Item
Standard Assessment Tool
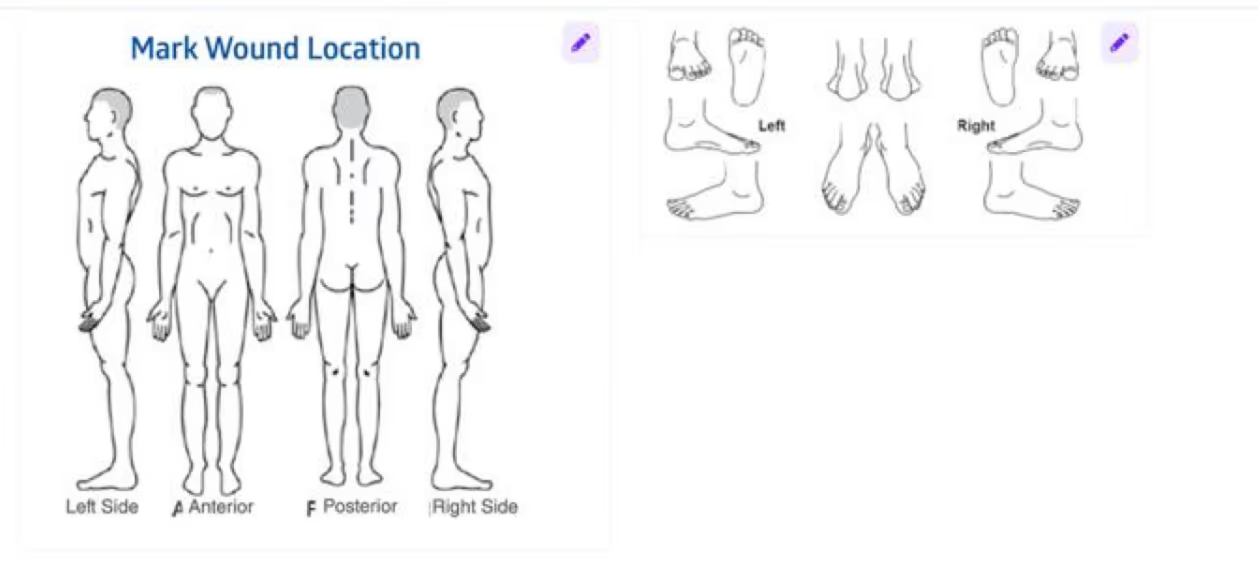
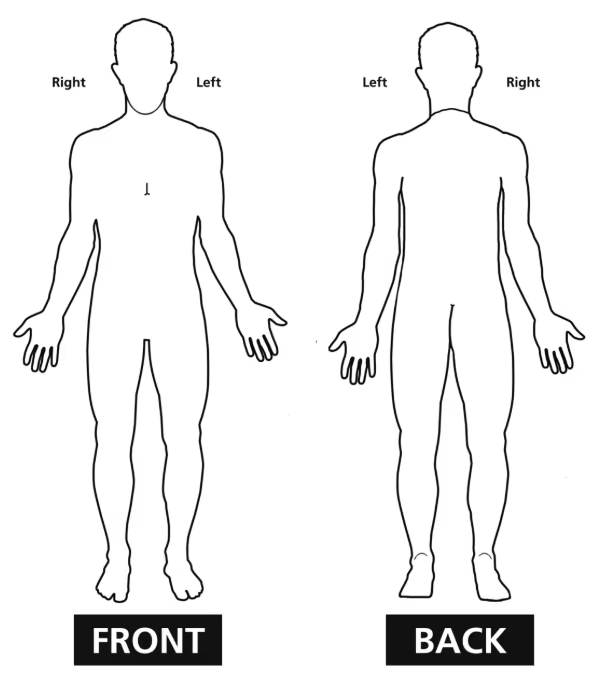
Wound Assessment +
Number
Location
TypeSelect
StatusSelect
Form Settings
GeneralAttributionDataCustom
Form NameStandard Assessment Tool
URLforms.aidbox.io/questionnaire/…
Version0.1.0
Status
DraftActiveRetiredUnknown
Appearance
Max width960px
QuestionnaireResponsePopulationData ExtractionNamed Expressions
Forms Demo / Forms
New UI
New Form
Template nameStatusVersionUpdatedAuthorActions
Formulario Agendamiento QX Bupa Santiago
interoperabilidad.bupa.cl/Questionnaire/qxflow
active1.0.018 JunBupa SantiagoInternational Patient Summary
forms.aidbox.io/questionnaire/ips
draft1.0.09 JunAtomica InformaticsROS — Review of Systems
forms.aidbox.io/questionnaire/ros
draft0.1.029 AprHealth SamuraiGAD-7
forms.aidbox.io/questionnaire/gad-7
draft0.1.030 MarHealth SamuraiVital Signs
forms.aidbox.io/questionnaire/vital-signs
draft0.1.030 MarHealth SamuraiPatient Knee Story
forms.aidbox.io/questionnaire/patient-knee-story
draft—27 May—16 forms50 / pageVersioned — every save is a new version
Forms Demo / Library
Wound
Any
MDS v3.0 - RAI v1.18.11 - Nursing home comprehensive (NC) item set
loinc.org/q/101105-5
MDS v3.0 - RAI v1.18.11 - Nursing home quarterly (NQ) item set
loinc.org/q/101106-3
MDS v3.0 - RAI v1.18.11 - Nursing home discharge (ND) item set
loinc.org/q/101107-1
MDS v3.0 - RAI v1.18.11 - Interim Payment Assessment (IPA)
loinc.org/q/101111-3
MDS v3.0 - RAI v1.18.11 - Swing bed PPS (SP) item set
loinc.org/q/101112-1
Wound Assessment Pnl
loinc.org/q/39135-9
Outcome and assessment information set (OASIS) — version B1
loinc.org/q/46462-8
MDS full assessment form — version 2.0
loinc.org/q/45981-8
Continuity assessment record — Acute care
loinc.org/q/52743-2
80 forms · Regenstrief Institute, Inc.
Wound Assessment
×
Body site
Wound bed and edge panel
Wound bed panel
Create new form
Import or convert
PDF to digital · AI-assisted
Consent for
Medical/Surgical Care/Emergency Treatment
and Child's Medical Information
Medical/Surgical Care/Emergency Treatment
and Child's Medical Information
In presenting my son/daughter for diagnosis and treatment
Name:for
Mother
Father
Legal Guardian
Son
Daughter
of years of age, hereby voluntarily consent to the rendering of such care, including diagnostic procedures, surgical and medical treatment and blood transfusions, by authorized members of the hospital staff or their designees, as may in their professional judgment be necessary.
I hereby acknowledge that no guarantees have been made to me as to the effect of such examinations or treatment on my child's condition.
I have read this form and certify that I understand its contents.
We/I hereby give our (my) consent to
(Name of Person/Agency)
who will be caring for our (my) child
(Name of Child)
for the period to to arrange for routine or emergency medical/dental care and treatment necessary to preserve the health of our (my) child.
We/I acknowledge that we are (I am) responsible for all reasonable charges in connection with care and treatment rendered during this period.
Name:
Family physician:
Address:
Pediatrician:
Telephone no.:
Surgeon:
Name of health insurance carrier:
Orthopedist:
Child's allergies, if any:
Group no.:
Date of last tetanus booster:
Agreement no.:
Medicines child is taking:
Signature:
Date:
Witness:
Date:
In case of emergency I can be reached at:
Import Questionnaire×
consent.pdf×
1234567891011121314151617181920212223242526
{
"resourceType": "Questionnaire",
"id": "consent-medical-surgical-emergency-child-medical-info",
"status": "draft",
"title": "Consent for Medical/Surgical Care/Emergency Treatment...",
"language": "en",
"item": [
{
"linkId": "sec-1",
"type": "group",
"text": "Consent for Medical/Surgical Care...",
"item": [
{
"linkId": "sec-1-intro",
"type": "display",
"text": "In presenting my son/daughter..."
},
{
"linkId": "sec-1-presenting-name",
"type": "text",
"text": "Name"
},
{
"linkId": "sec-1-presenting-for",
"type": "text",
"text": "for"
AI SettingsSubmit
Extracted in 3.2sQuestionnaire/consent-medical-surgical-emergency-child-medical-info